

Calcified coronary lesions are increasingly common during percutaneous coronary intervention (PCI). Treatment of refractory calcified lesions are usually challenging and needs meticulous calcium preparation tools including intravascular lithotripsy , serial high-pressure balloon inflations, advanced imaging (such as optical coherence tomography, OCT, etc) and failure to treat those lesions is often associated with worse major cardiovascular outcomes (MACE)(1). In recent years, randomised controlled trials comparing different strategies of calcium modification tools remain controversial and debated. However, this innovative randomised multi-centre ‘VICTORY’ trial aims to answer the questions around the non-inferiority of one simple type of strategy, super high-pressure OPN-noncompliant balloon (NCB) over commonly used intravascular lithotripsy (IVL). (2)
This is the first study to compare the efficacy and safety of the OPN balloon versus IVL for preparing heavily calcified coronary artery lesions(2) . The trial includes a total of 282 patients with angiographically significant and severe calcification lesions. The extent of calcium burden was assessed through angiography and/or optical coherence tomography(OCT). The stent expansion was also assessed by OCT . The study was randomised into 1:1 ratio and classified into either OPN NCB or IVL arm and meticulously followed up in 30 days. Lesions were carefully prepared with either OPN NCB or IVL tool, then treated meticulously with drug eluting stent (DES, everolimus- or zotarolimus-eluting stents). Then post-PCI imaging assessed with OCT at the end. All patients were followed up in 30 days. The primary endpoints include stent expansion after OCT-guided PCI , and the clinical outcomes comprise of target vessel failure (TVF composite : cardiovascular deaths, stent thrombosis, target vessel revascularization, TVR) at 30 days. There was no statistical significance in the primary endpoint of stent expansion between two calcium tools with similar procedural outcomes (OPN 85% Vs IVL 84% ) , p value for non-inferiority noted as <0.001, superiority not met ( difference in medians :1.0(95% CI -2.45 to 4.45), p for superiority 0.570).
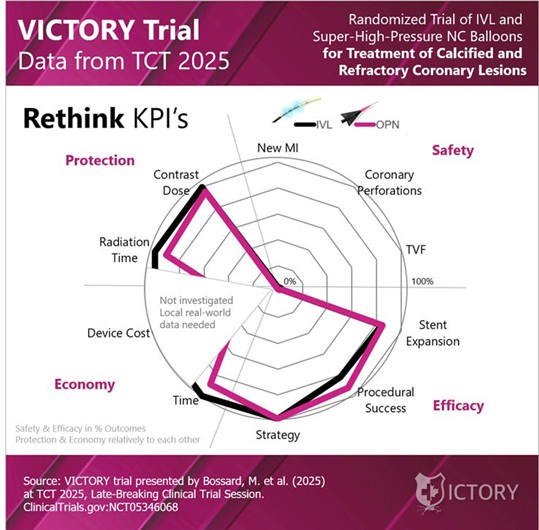
In summary, super-high-pressure non-compliant (NC) balloons are non-inferior to intravascular lithotripsy (IVL) in severely calcifed coronary lesions, with similar safety profile. There is a limitation in this trial that it only includes two large demographic areas only with heavily expert operators-dependent, and the study is not powered for clinically relevant outcomes with OCT-guided stent expansion in calcified lesions (which is not as commonly feasible as angiography or intravascular ultrasound. Nevertheless, this VICTORY trial has clearly demonstrated other economic perspectives when preparing and treating calcified lesions, as super-high-pressure balloon(OPN) is considered as a lower-cost alternative strategy compared to intravascular lithotripsy (IVL) and a faster solution to some clinical settings in real world practice.(1,2)
The diagram below summarizes the VICTORY trial (rethink KPIs in IVL Vs OPN) (copyright permission taken and credit to TCT 2025)
References
1. Kladou E, Williford NN, Kathri J, Kumar G, Nathan S, Patel N, Reed G, Seto A, Shlofmitz E, Rinfret S, Hall A. Best practices for use of the super high pressure OPN balloon. The American Journal of Cardiology. 2026 Feb 1.
2. Bossard M. A Randomized, Multicenter, Non-Inferiority Comparison of Intravascular Lithotripsy and Super-High-Pressure Non-Compliant Balloons for Treatment of Calcified and Refractory Coronary Lesions – the VICTORY trial. San Francisco, CA: Paper presented at: Transcatheter Cardiovascular Therapeutics (TCT) 2025, October 26, 2025

Author Sub-editor: Dr Pok-Tin Tang Dr Pok-Tin Tang is an ST5 cardiology registrar in the Thames Valley deanery, currently undertaking a period of out of

Author Sub-editor: Dr May Hu Dr May Hu is a cardiology trainee in the North West deanery. She graduated with First Class Honours from the University

Author Sub-editor: Dr Jhiamluka Solano Dr Jhiamluka Solano is a cardiology resident doctor (ST6) in the Yorkshire and Humber Deanery, currently undertaking a DPhil (PhD)

Author Sub-editor: Dr Joshua Rowland Dr Joshua Rowland is a cardiology registrar working in the North West Deanery. He graduated from the University of Manchester

Author Sub-editor: Dr Atmadeep Banerjee Dr Atmadeep Banerjee is an ST4 Cardiology Registrar in the Kent, Surrey and Sussex deanery. He graduated from Calcutta National