

The emerging role of treating vulnerable plaques as a preventative revascularisation strategy is highlighted in the PREVENT Trial1. With the contemporary use of intravascular imaging modalities such as intravascular ultrasound (IVUS) and optical coherence tomography (OCT), features of plaque vulnerability including thin capped fibroatheroma (TCFA), large necrotic core, positive remodelling and high plaque burden have been shown to be associated with an increased risk of future major adverse cardiovascular events (MACE)².
The main objective of the PREVENT study was to assess whether preventive percutaneous coronary intervention (PCI) of non-flow limiting vulnerable plaques improves clinical outcomes compared with optimal medical therapy (OMT) alone. The primary outcome was a composite of death from cardiac causes, target-vessel myocardial infarction, ischaemia-driven target-vessel revascularisation, or hospitalisation for unstable or progressive angina, at 2 years after randomisation1.
Table 1 summarises the PICO (Population, Intervention, Control, Outcome) framework of ‘PREVENT’ Trial.
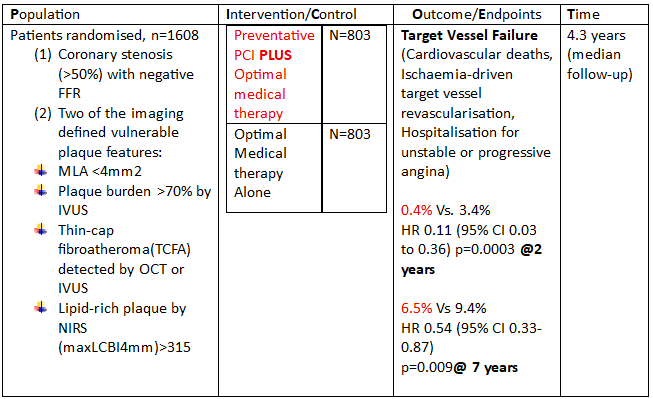
FFR= Fractional Flow Reserve
PCI= Percutaneous coronary intervention
HR= Hazard Ratio
CI=Confidence Interval
p-value- <0.05- clinically significant
MLA- Minimal Luminal Area
TVR= Target-vessel failure
IVUS- Intra-vascular Ultrasound
OCT= Optical Coherence Tomography
NIRS= Near-Infrared Spectroscopy
PREVENT represents the first investigator-initiated, open-label, randomised controlled trial specifically designed to evaluate preventive PCI of non-flow-limiting vulnerable plaques in addition to guideline directed OMT. The longstanding clinical dilemma, whether to intensify systemic therapy alone or to pre-emptively seal high-risk plaques, remains unresolved. PREVENT demonstrated a significant reduction in the composite primary endpoint at two years, an effect sustained during longer-term follow-up. However, this benefit was largely driven by reductions in ischaemia-driven target vessel revascularisation, with very low absolute rates of cardiac death and myocardial infarction in both groups.
While these findings suggest that focal treatment of selected high-risk plaques may confer incremental benefit beyond contemporary OMT, important considerations remain, including low overall event rates, imbalance in dual antiplatelet therapy exposure, imaging-based lesion selection, and limited generalisability beyond predominantly East Asian populations. Further adequately powered, multi-centre randomised trials and real-world registry data are required before preventive PCI of non-obstructive vulnerable plaques can be adopted as routine clinical practice
1. Park SJ, Ahn JM, Kang DY, Yun SC, Ahn YK, Kim WJ, Nam CW, Jeong JO, Chae IH, Shiomi H, Kao HL. Preventive percutaneous coronary intervention versus optimal medical therapy alone for the treatment of vulnerable atherosclerotic coronary plaques (PREVENT): a multicentre, open-label, randomised controlled trial. The Lancet. 2024 May 4;403(10438):1753-65.
2. Libby P, Pasterkamp G, Crea F, Jang IK. Reassessing the mechanisms of acute coronary syndromes: the “vulnerable plaque” and superficial erosion. Circulation research. 2019 Jan 4;124(1):150-6

Author Sub-editor: Dr Joshua Rowland Dr Joshua Rowland is a cardiology registrar working in the North West Deanery. He graduated from the University of Manchester

Author Sub-editor: Dr Atmadeep Banerjee Dr Atmadeep Banerjee is an ST4 Cardiology Registrar in the Kent, Surrey and Sussex deanery. He graduated from Calcutta National


Authors Heartbeat Sub-Editor: Sandeep Singh Dr Sandeep Singh is a Cardiology Clinical Fellow at Nottingham University Hospitals NHS Trust. After graduating from India, he completed
