
Headline results in early 2026 come from IVORY and IVORY-FINALE, phase-2 trials testing if immune modulation after acute MI can cut recurrent risk.i,ii
Inflammation is known to fuel post-MI events, so selectively boosting regulatory T cells (Tregs) with low-dose interleukin-2 (aldesleukin) aims to “cool” arterial inflammation without broad immunosuppression.iii
IVORY was a randomised, double-blind, placebo-controlled study in patients soon after ACS who were treated for ~8 weeks with low-dose aldesleukin (interleukin-2) vs. placebo. Sixty patients were enrolled, with IVORY-FINALE providing longer follow-up for clinical events.
Compared to placebo, the primary biological outcome, ‘arterial inflammation’ fell by ~8% on FDG-PET/CT with low-dose IL-2. The effect was greater in the most inflamed arterial segments (−8.3%; P=0.009). Treatment also increased Treg cell levels compared to placebo (P < 0.0001).
Over ~2 years, no MACE were observed in the IL-2 group, compared to three events (≈11%) in placebo group; although this is an encouraging signal, the study was underpowered for definitive conclusions regarding long-term clinical outcomes. Safety was reassuring, with adverse events broadly similar to placebo.
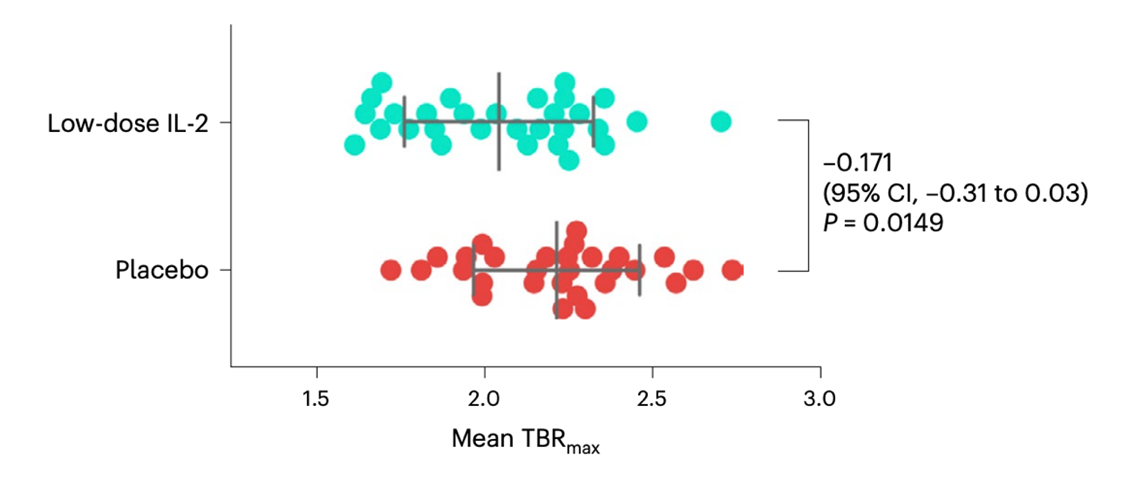
Figure: Primary endpoint. Arterial inflammation in the index vessel at end of 8-week treatment as quantified by FDG PET-CT: low-dose IL-2 (n=31) vs placebo (n=29). Arterial inflammation was −0.171 (7.7%) lower in the low-dose IL-2 group compared to placebo (P = 0.0149). Dots = individual patients; long vertical line = group mean; error bars = standard deviation.
Secondary prevention after MI has long centred on antiplatelets, statins and BP control. IVORY and IVORY-FINALE propose a potential fourth tool in the armamentarium: targeted immune therapy. These findings indicate some mechanistic plausibility with the potential for clinical efficacy. By selectively boosting Tregs and calming maladaptive post-infarct immunity without broad (systemic) immunosuppression, low-dose IL-2 may offer a precise way to “turn down” vascular inflammation. The investigators argue this could reduce recurrent atherothrombotic events if validated at scale.
This indication for low-dose IL-2 therapy is not imminent in routine clinical practice, it could one day be part of our clinical took kit for more personalised post-MI care for patients with residual inflammation. Confirmation in larger, outcomes-powered phase-3 trials, as well as patient phenotyping for therapy selection is required. Until then, these data should be viewed as proof-of-mechanism with promising but preliminary clinical implications – watch this space.
https://www.nature.com/articles/s41591-025-04090-y
https://bmjopen.bmj.com/content/12/10/e062602
References
i Sriranjan RS, Zhao TX, Kostapanos M, et al. Anti-inflammatory therapy with low-dose interleukin-2 in acute coronary syndromes (IVORY): a randomized, double-blind, placebo-controlled phase 2 trial. Nature Medicine. 2026. doi:10.1038/s41591-025-04090-y.
ii Low-Dose IL-2 for the Reduction of Vascular Inflammation in Acute Coronary Syndromes — Clinical Outcomes & Follow-up (IVORY-FINALE). ClinicalTrials.gov Identifier: NCT06427694. Health Research Authority study summary available.
iii Ridker PM, Everett BM, Thuren T, et al. Relationship of C-reactive protein reduction to cardiovascular event reduction following treatment with canakinumab: a secondary analysis from CANTOS. Lancet. 2017;390:1833-1842. doi:10.1016/S0140-6736(17)32290-0.