RATIONALE:
Atrial fibrillation/flutter (AF) is increasingly recognised as a clinically significant complication of transthyretin cardiac amyloidosis (ATTR‑CA). Progressive infiltration of atrial cardiomyocytes by amyloid fibrils underpins the pathophysiology, leading to structural and electrical remodelling of the atria. Understanding the predictors and burden of AF in this population is essential for targeted monitoring and management.
METHODS:
Chan et al1. conducted a single‑centre cohort study of 419 patients with ATTR‑CA. Baseline AF status, demographic and clinical characteristics, including amyloid stage per the National Amyloidosis Centre (NAC) and Columbia score, were recorded. Longitudinal follow-up captured incident AF events, with rhythm surveillance via ECG, extended monitoring, and device interrogation. Multivariable models assessed predictors of AF incidence, and the impact of tafamidis therapy was evaluated.
RESULTS:
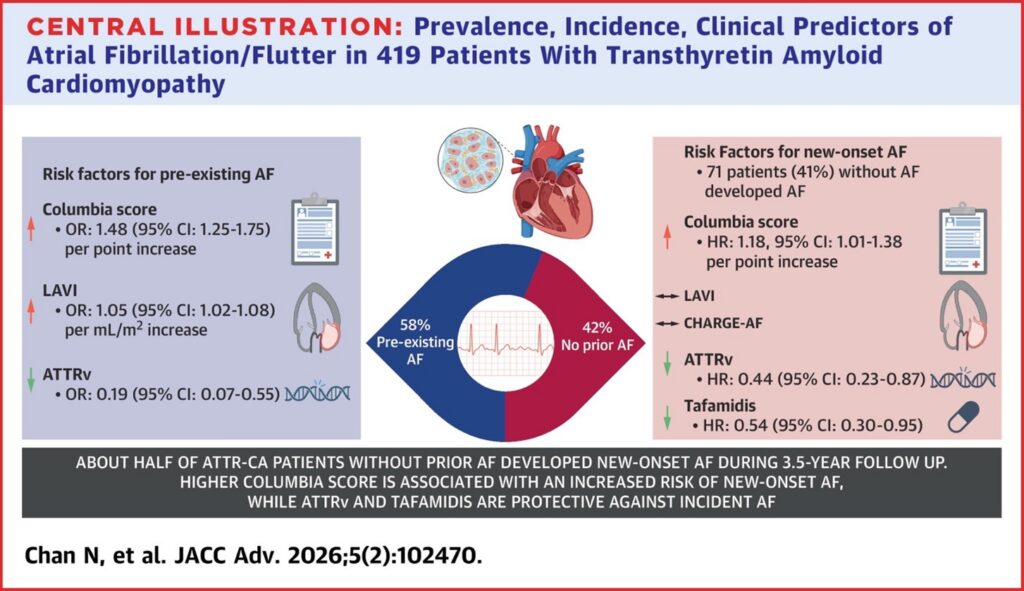
At presentation, 58% of patients had AF, rising to 75% when incident events during follow-up were included. Pre-existing AF clustered with wild-type ATTR (ATTRwt), worse NYHA functional class (III–IV), and higher NAC amyloid stage. Independent predictors included higher Columbia score (OR 1.48 per point, 95% CI 1.25–1.75; P < 0.0001) and larger left atrial volume index (LAVI) (OR 1.05 per mL/m², 95% CI 1.02–1.08; P < 0.0001), while hereditary ATTR (ATTRv) was protective (OR 0.19, 95% CI 0.07–0.55; P = 0.002).
Among 175 patients in sinus rhythm at baseline, 41% developed new-onset AF over a median of 2 years. Each point increase in Columbia stage conferred an 18% higher hazard of incident AF. The CHARGE-AF score failed to discriminate risk, and LAVI lost significance in multivariable models, emphasising disease stage as the stronger predictor. Tafamidis therapy was associated with a 46% relative reduction in incident AF (HR 0.54, 95% CI 0.30–0.95), and ATTRv genotype also conferred protection (HR 0.44, 95% CI 0.23–0.87).
DISCUSSION:
AF in ATTR‑CA is common, closely linked to disease stage, and often predates clinical recognition. Standard population-based AF risk scores are insufficient; amyloid-specific staging better identifies patients at risk. The observed association between tafamidis and lower incident AF suggests a potential disease-modifying effect on atrial remodelling, complementing its established benefits on survival and heart failure outcomes.
Clinical implications:
- Incorporate AF surveillance into routine ATTR‑CA care, particularly in patients with higher Columbia stage.
- Recognise AF as a marker of advanced disease, warranting early diagnosis and timely initiation of disease-modifying therapy.
- As tafamidis adoption increases, arrhythmic outcomes should be prospectively captured in registries to validate these findings and guide preventive strategies.
Reference:
Chan N, Brailovsky Y, Teruya S, Mirabal A, Weinsaft AY, De Los Santos J, Guadalupe S, Jimenez M, Helmke S, Cuomo M, Smiley D, Biviano A, Dizon J, Wan E, Yarmohammadi H, Maurer MS. Atrial Fibrillation/Flutter in Transthyretin Cardiac Amyloidosis: Prevalence, Incidence, Clinical Predictors, and Effect of Tafamidis. JACC Adv. 2025 Dec 24;5(2):102470. doi: 10.1016/j.jacadv.2025.102470. Epub ahead of print. PMID: 41448121; PMCID: PMC12800393.