
Can we stop treating atrial fibrillation-induced heart failure?
Author Sub-editor: Dr Joshua Rowland Dr Joshua Rowland is a cardiology registrar working in the North West Deanery. He graduated from the University of Manchester

Coffee is one of the most ubiquitously consumed substances worldwide and is Europe’s most popular caffeinated drink (1). Conventional wisdom would surmise that coffee (and caffeine-containing products) exerts a pro-arrhythmic effect (2). Established notions exist that coffee can contribute to atrial fibrillation (AF), and/or trigger AF episodes (3). “So, can I still drink coffee?” is one of the commonest questions posed to clinicians around the world during AF-related consultations. The first randomised assessment of coffee on AF outcomes, the DECAF (Does Eliminating Coffee Avoid Atrial Fibrillation?) trial, aims to provide more definitive information between coffee consumption and atrial arrhythmia.
Some observational studies support this link between caffeine and triggering AF (4,5). That being said, the relationship between coffee/caffeine and atrial arrhythmia has not been clearly elucidated. Other observational studies have demonstrated that the jury is still out when it comes to the relationship between caffeine consumption and AF with results spanning the entire spectrum from harmful to beneficial (6) with neutral (7) effects in between; so, a unified consensus on the relationship between the two is overdue.
The DECAF trial was a prospective open-label international multicentre RCT. Inclusion criteria were: patients >21 years, planned DCCV for sustained AF or atrial flutter, chronic coffee consumption and willingness to adhere to either coffee abstinence or continuation, depending on randomisation. Randomisation, occurring after DCCV, was 1:1 to either caffeinated coffee consumption or abstinence from coffee and all potentially caffeine containing items (i.e. decaffeinated coffee, tea and chocolate). Follow-up, via telephone, video call or in-person site visit, occurred at 1,3- and 6-months post randomisation. The primary endpoint was the clinically detected recurrence of AF or atrial flutter lasting 30 seconds or longer assess in a time-to-event analysis, via an intention-to-treat analysis.
After applying exclusions, a total of 200 patients were randomly assigned to consumption of coffee post DCCV (100 patients) or caffeine abstinence. Baseline characteristics were largely balanced between groups, however there was numerical imbalances in sex, coronary artery disease prior AF ablation. Approximately half of enrolled patients were taking antiarrhythmic medication.
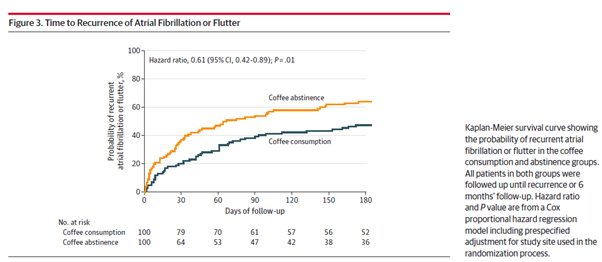
Average coffee consumption in the coffee group was 7 (IQR 6-11) cups per week. Time to recurrence was longer in the coffee consumption group than in the abstinence group leading to a 39% lower hazard of AF recurrence with consumption (HR, 0.61 {95% CI, 0.42-0.89}; P=0.01). This benefit appeared to be consistent across subgroups except for ablation history (P=0.04). Adherence from consuming any coffee was 69% per cent in the abstinence group.
The results the DECAF trial demonstrate that patients who drink coffee regularly went longer before developing recurrence of AF than those who abstained. One possible mechanism for this effect is that adenosine facilitates AF induction, and caffeine consumption contributes to the blocking of A1 and A2 adenosine receptors which has a potential antiarrhythmic effect (8,9). The findings of DECAF supports some of observational studies that caffeine can have a protective effect against atrial arrhythmia recurrence, and that coffee consumption in moderation may not be harmful with respect to AF recurrence. Clinicians will find these implications useful to draw on when having nuanced, balanced discussions about on-going caffeine consumption with patients living with atrial arrythmias.
REFERENCES:
Author Sub-editor: Dr Joshua Rowland Dr Joshua Rowland is a cardiology registrar working in the North West Deanery. He graduated from the University of Manchester

Authors Heartbeat Sub-Editor: Anindya Mukherjee Dr. Anindya Mukherjee is a ST5 trainee registrar in Cardiology at Mid Yorkshire Teaching NHS Trust, UK, with extensive experience
